
We established in Part 1 that our heart needs a controlled electrical signal to work. Here we talk about the different types of rhythm, which ones can be shocked with a defibrillator and why we sometimes cannot shock a heart.
In part 1 we showed that each part of the heart receives an electrical impulse in sequence to cause its muscle to contract. This impulse can be measured by placing a voltmeter across the heart and measuring the signal that it generates over a time period. We may know it better as the ‘sticky dots’ that are put on a patient’s chest or limbs (either in real life or on medical programmes on television). These are connected to a machine that can measure and display these signals. Anyone trained can look at these signals to see what they represent, however, anyone that has watched any type of medical drama should be able to recognise one or two of them anyway
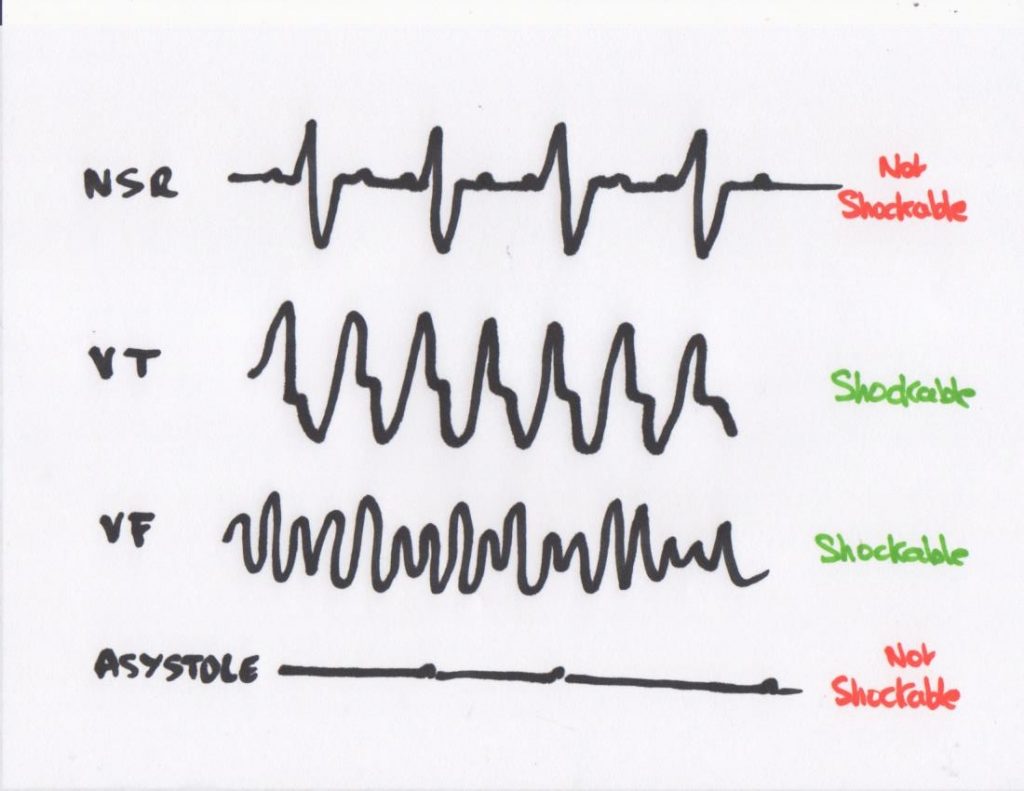
This image shows four of the main rhythms that a heart may be in. There are others and there are variations on the above, but let’s concentrate on these. Clearly this is not a precise interpretation, nor degree-level analysis, however a broad understanding of these rhythms will be useful in what follows.
Number 1 – NSR or Normal Sinus Rhythm. This is what a heart looks like when it is beating normally. It’s what you see on the opening credits of some medical dramas and on the screens of defibrillators when a person is healthy or has had their heart ‘restarted’
Number 2 – Ventricular tachycardia. This is what you see when a heart is beating abnormally fast. As the heart chambers need to refill with blood between beats, if it is beating too fast, this doesn’t happen, blood does not get circulated and this is life-threatening.
Number 3 – Ventricular fibrillation. This is electrical ‘anarchy’ in the heart. Remember we said that everything happens in sequence? Well, it can get out of sequence and this is the result. The heart’s chambers are not contracting and expanding and so blood is not being squeezed around the body.
Number 4 – Asystole. In medical-speak, ‘a-‘ or ‘an-‘ means ‘lack of’ and ‘systole’ comes from the Greek for ‘contraction’. It is the total absence of any discernible rhythm. There is no electrical activity (possibly the odd small blip)
Fact of the Day. A defibrillator stops the heart’s electrical activity, it does not start it!
What does this mean in real life? Firstly, if a heart is in asystole (“flatline”), there is no electrical activity and so nothing to stop. Your defibrillator can detect this rhythm and will refuse to shock the patient. Secondly as it ‘knows’ what each of the rhythms look like, if it detects a ‘normal’ heart rhythm (NSR) it will refuse to shock that. No point stopping the electrical activity if it looks normal! It is only if it recognises VT or VT activity that it will allow you to shock it.
Techy bit: One other rhythm worth a mention is Pulseless Electrical Activity (“PEA” – also used to be called electromechanical dissociation – “EMD”). Normally an electrical signal will cause the heart muscle to contract. In PEA the electrical activity is there, but the heart is not beating. A defibrillator cannot tell the difference between this and a normal rhythm and will refuse to shock, even though the patient does not have a pulse.
When you attach defibrillator pads to a patient it will analyse the rhythm and make a decision based on what it finds. It is important to see that there are a number of reasons why it will choose not to shock. If you have been carrying out Cardio Pulmonary Resuscitation (CPR) and it chooses not to shock, it is not a reflection on the quality of your CPR, it is simply that it has detected a rhythm that it cannot shock. Two minutes later, when it reanalyses, it may be a different decision.


Be the first to comment